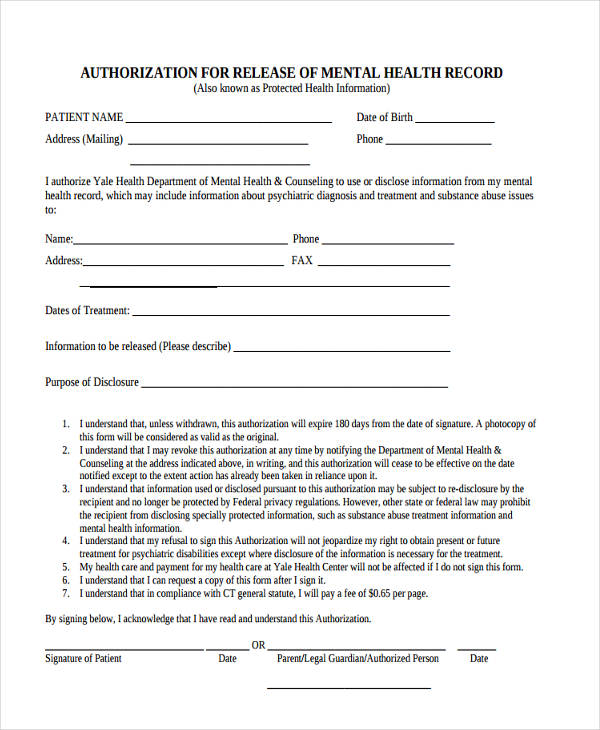
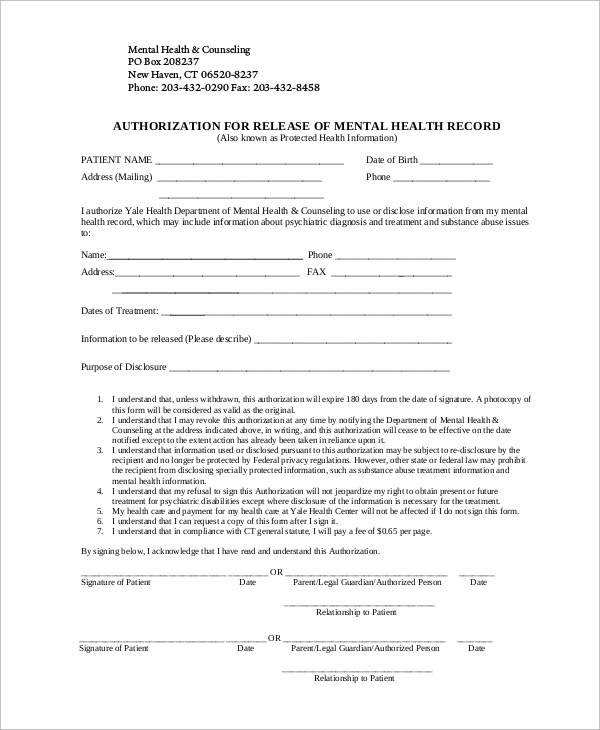
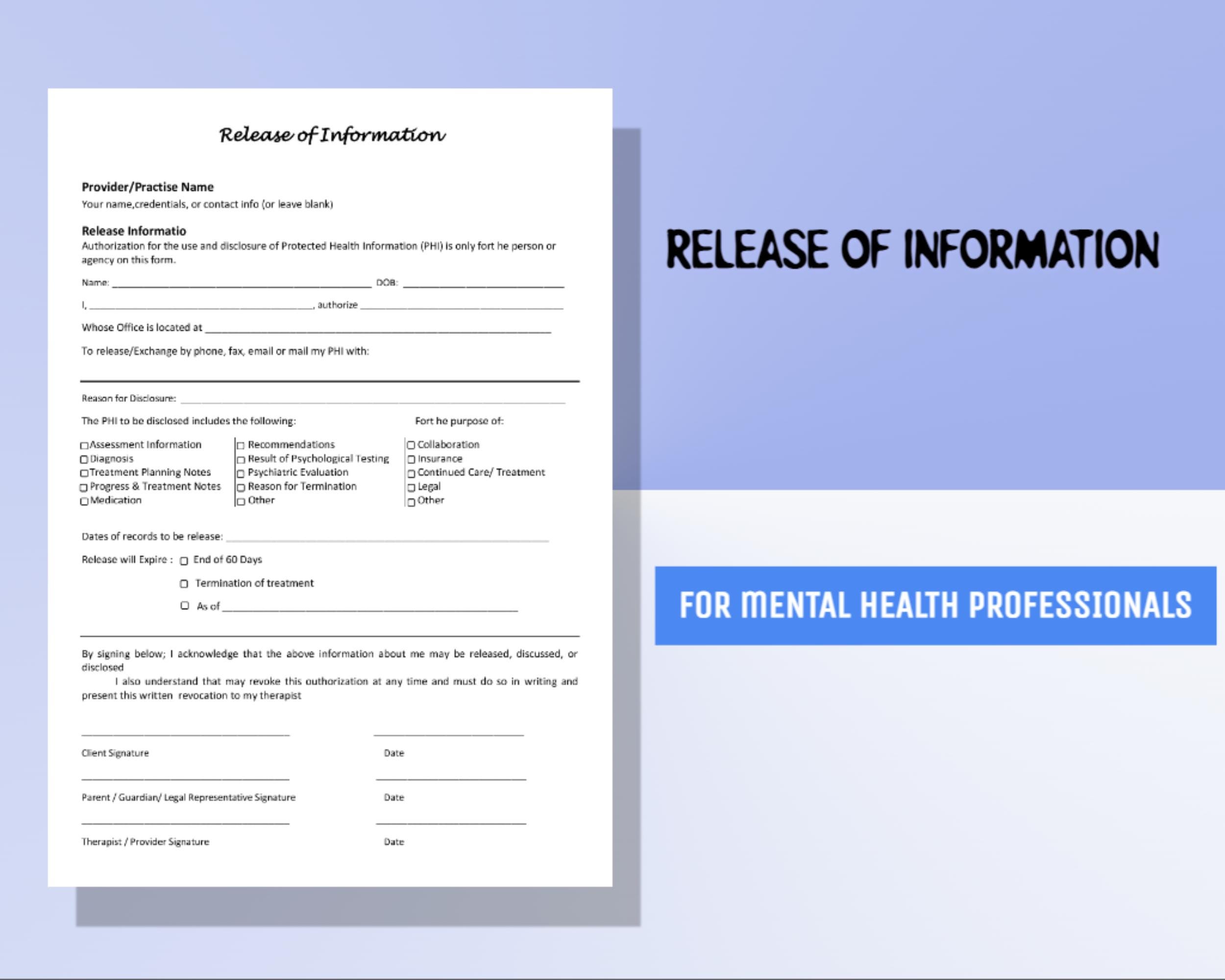
Release Of Information Template For Mental Health - By signing below, i authorize the release. And/or hipaa 45 cfr) and state. That my signing of this authorization is voluntary. I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. Of my information as specified above. And/or hipaa 45 cfr) and state. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I am giving my permission to compass health to disclose my confidential health records.
My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; And/or hipaa 45 cfr) and state. And/or hipaa 45 cfr) and state. I am giving my permission to compass health to disclose my confidential health records. Of my information as specified above. That my signing of this authorization is voluntary. I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. By signing below, i authorize the release.
That my signing of this authorization is voluntary. By signing below, i authorize the release. Of my information as specified above. And/or hipaa 45 cfr) and state. I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. I am giving my permission to compass health to disclose my confidential health records. And/or hipaa 45 cfr) and state. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2;
Mental Health Release of Information Form, ROI, PDF, Fillable, Editable
Of my information as specified above. I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; My health information is protected by federal regulation (alcohol & drug abuse patient records, 42.
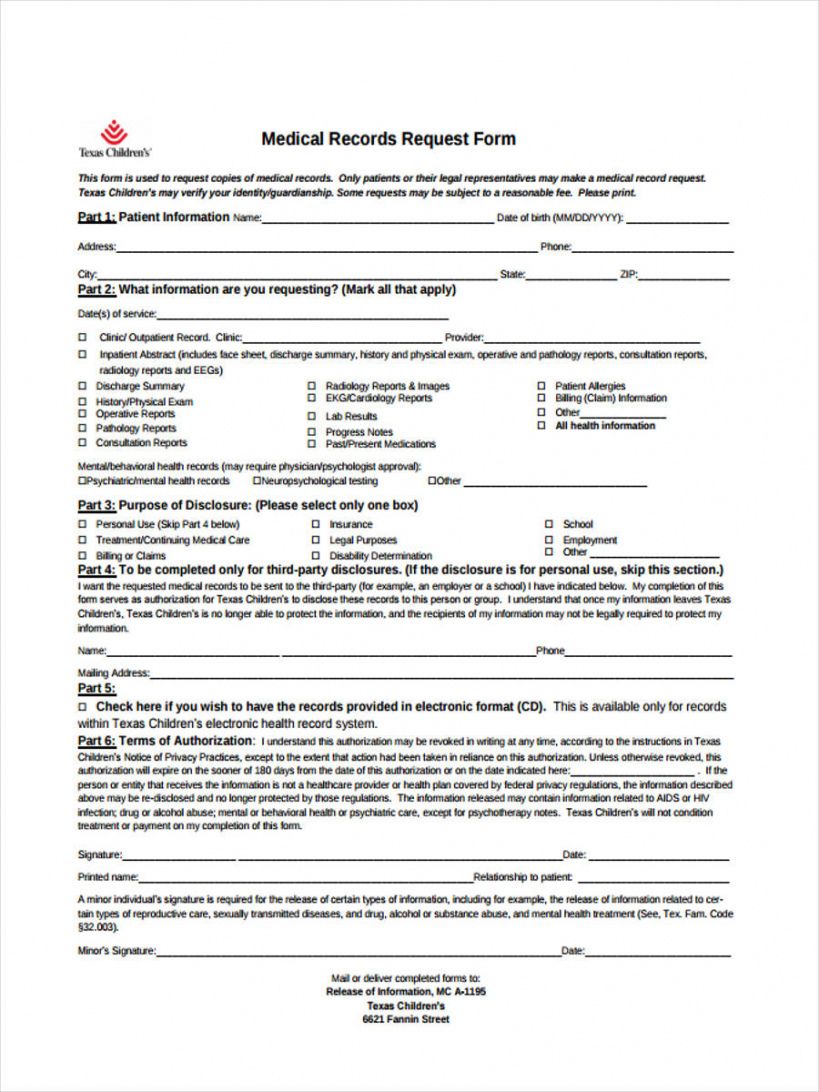
FREE 22+ Release of Information Form Samples, PDF, MS Word, Google Docs
I am giving my permission to compass health to disclose my confidential health records. I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. By signing below, i authorize the release. Of my information as specified above. And/or hipaa 45 cfr) and state.
Release Of Information Form Template Mental Health
And/or hipaa 45 cfr) and state. That my signing of this authorization is voluntary. I am giving my permission to compass health to disclose my confidential health records. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I understand that my medical records may contain information regarding the diagnosis or treatment.
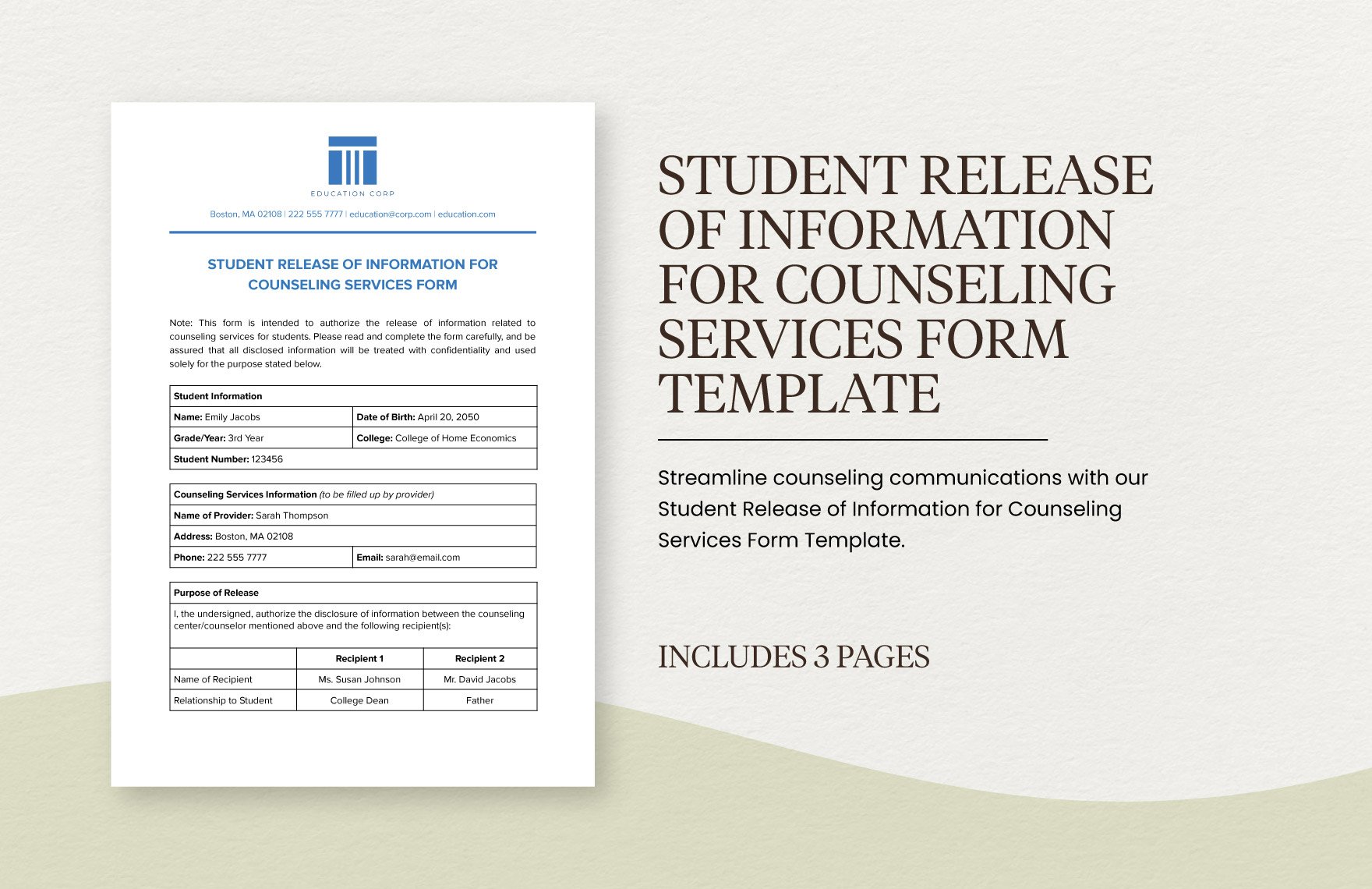
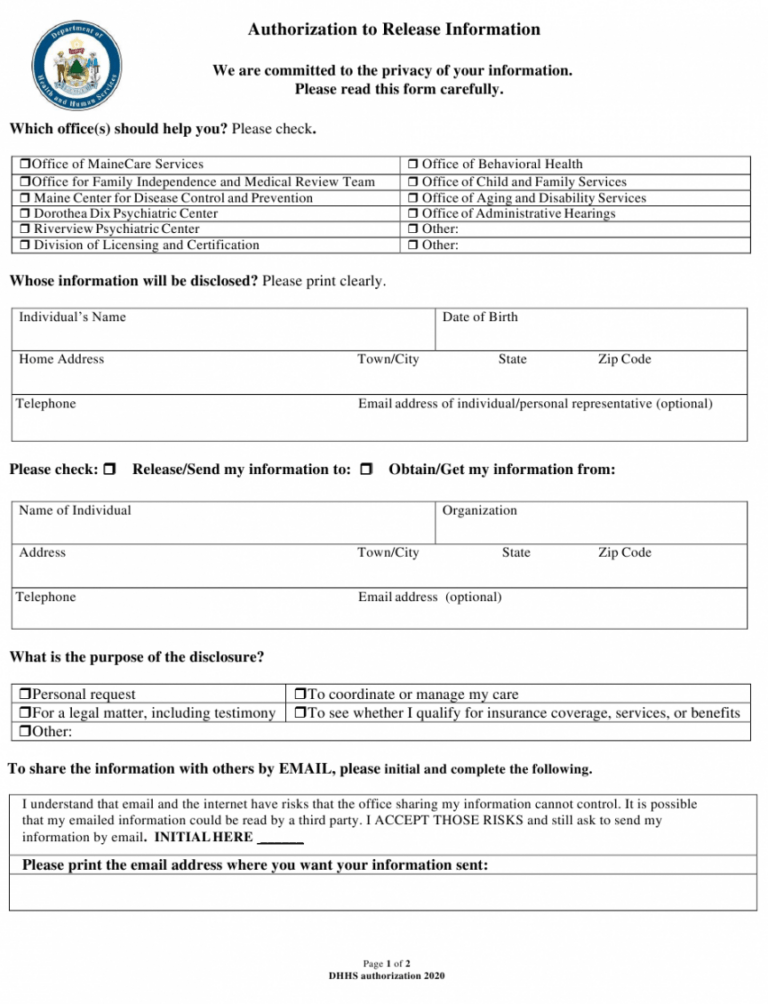
Editable Student Form Templates in PDF to Download
I am giving my permission to compass health to disclose my confidential health records. And/or hipaa 45 cfr) and state. I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. Of my information as specified above. That my signing of this authorization is voluntary.
Release Of Information Form Mental Health Template
My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I am giving my permission to compass health to disclose my confidential health records. And/or hipaa 45 cfr) and state. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; And/or hipaa 45 cfr).
Mental Health Release of Information Form, ROI, PDF, Fillable, Editable
I am giving my permission to compass health to disclose my confidential health records. And/or hipaa 45 cfr) and state. And/or hipaa 45 cfr) and state. I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. Of my information as specified above.
Free Release Of Information Form Mental Health Template Doc
I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. I am giving my permission to compass health to disclose my confidential health records. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; And/or hipaa 45 cfr) and state. And/or.

Mental Health Release Of Information Form & Template Free PDF Download
My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I am giving my permission to compass health to disclose my confidential health records. That my signing of this authorization is voluntary. And/or hipaa 45 cfr) and state. I understand that my medical records may contain information regarding the diagnosis or treatment.
Release of Info Mental Health ROI Privacy Paperwork Release of
My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; And/or hipaa 45 cfr) and state. That my signing of this authorization is voluntary. By signing below, i authorize the release. And/or hipaa 45 cfr) and state.
Release Of Information Form Template Mental Health
That my signing of this authorization is voluntary. And/or hipaa 45 cfr) and state. Of my information as specified above. My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,.
By Signing Below, I Authorize The Release.
My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; I understand that my medical records may contain information regarding the diagnosis or treatment of drug and/or alcohol abuse, substance abuse,. That my signing of this authorization is voluntary. I am giving my permission to compass health to disclose my confidential health records.
And/Or Hipaa 45 Cfr) And State.
My health information is protected by federal regulation (alcohol & drug abuse patient records, 42 cfr part 2; Of my information as specified above. And/or hipaa 45 cfr) and state.