Medication Authorization Form - I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. Failure to complete this form in its entirety may result in delayed processing or an adverse. I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. Certain plans and situations may require. This form is based on express scripts standard criteria and may not be applicable to all patients;
Failure to complete this form in its entirety may result in delayed processing or an adverse. I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. This form is based on express scripts standard criteria and may not be applicable to all patients; I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. Certain plans and situations may require.
This form is based on express scripts standard criteria and may not be applicable to all patients; I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. Certain plans and situations may require. Failure to complete this form in its entirety may result in delayed processing or an adverse.

Fillable Online Medication Administration Authorization Form.pdf Fax
I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. Certain plans and situations may require. Failure to complete this form in.

Medication Authorization Form Monticello Middle School
This form is based on express scripts standard criteria and may not be applicable to all patients; I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request.
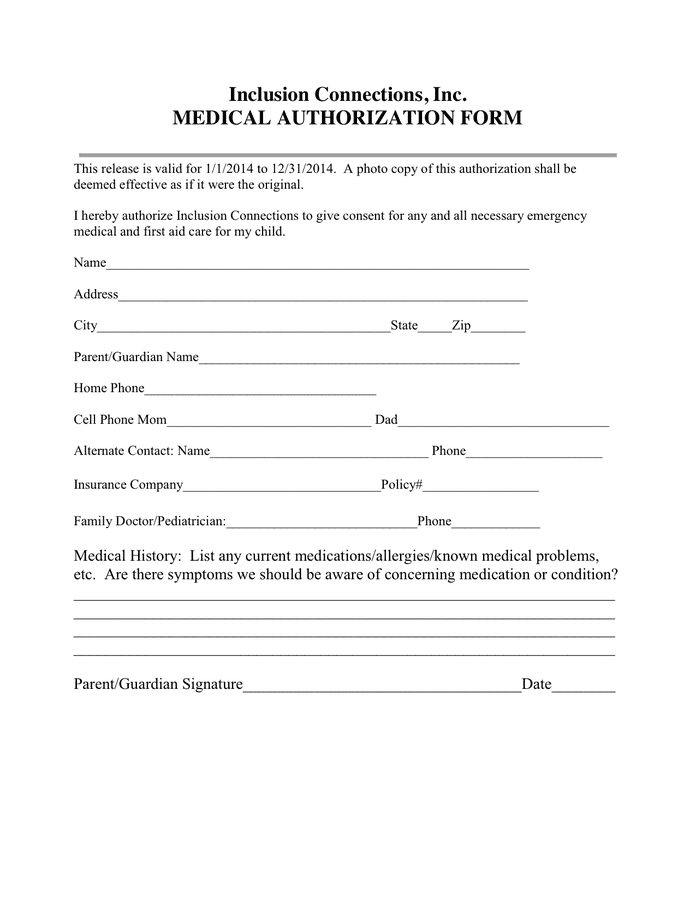
Medical Authorization Form download free documents for PDF, Word and
Certain plans and situations may require. This form is based on express scripts standard criteria and may not be applicable to all patients; I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. Failure to complete this form in its entirety may result in delayed processing.

MD School Medication Administration Authorization Form 20042022 Fill
This form is based on express scripts standard criteria and may not be applicable to all patients; Certain plans and situations may require. Failure to complete this form in its entirety may result in delayed processing or an adverse. I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical.
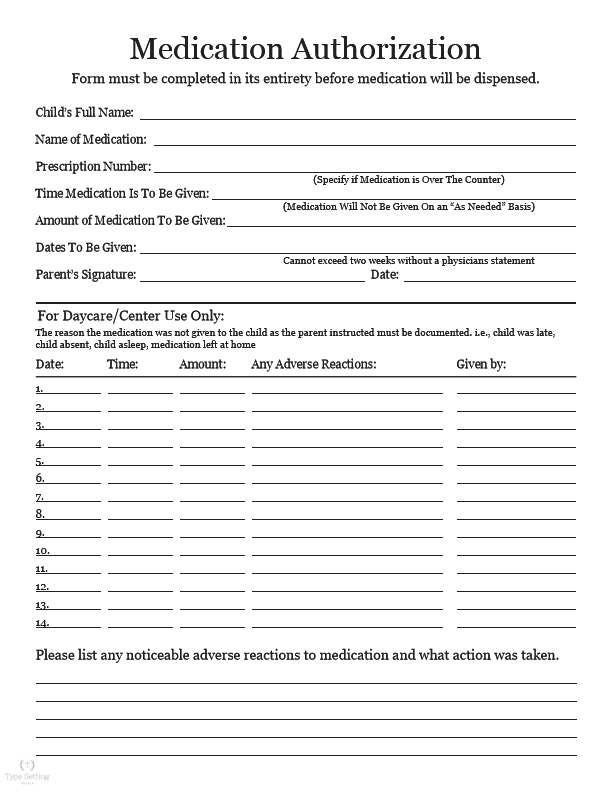
Medication Authorization Form Instant Digital Download Etsy Australia
This form is based on express scripts standard criteria and may not be applicable to all patients; I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. Certain plans and situations may require. I understand that the health plan, insurer, medical group or its designees may.
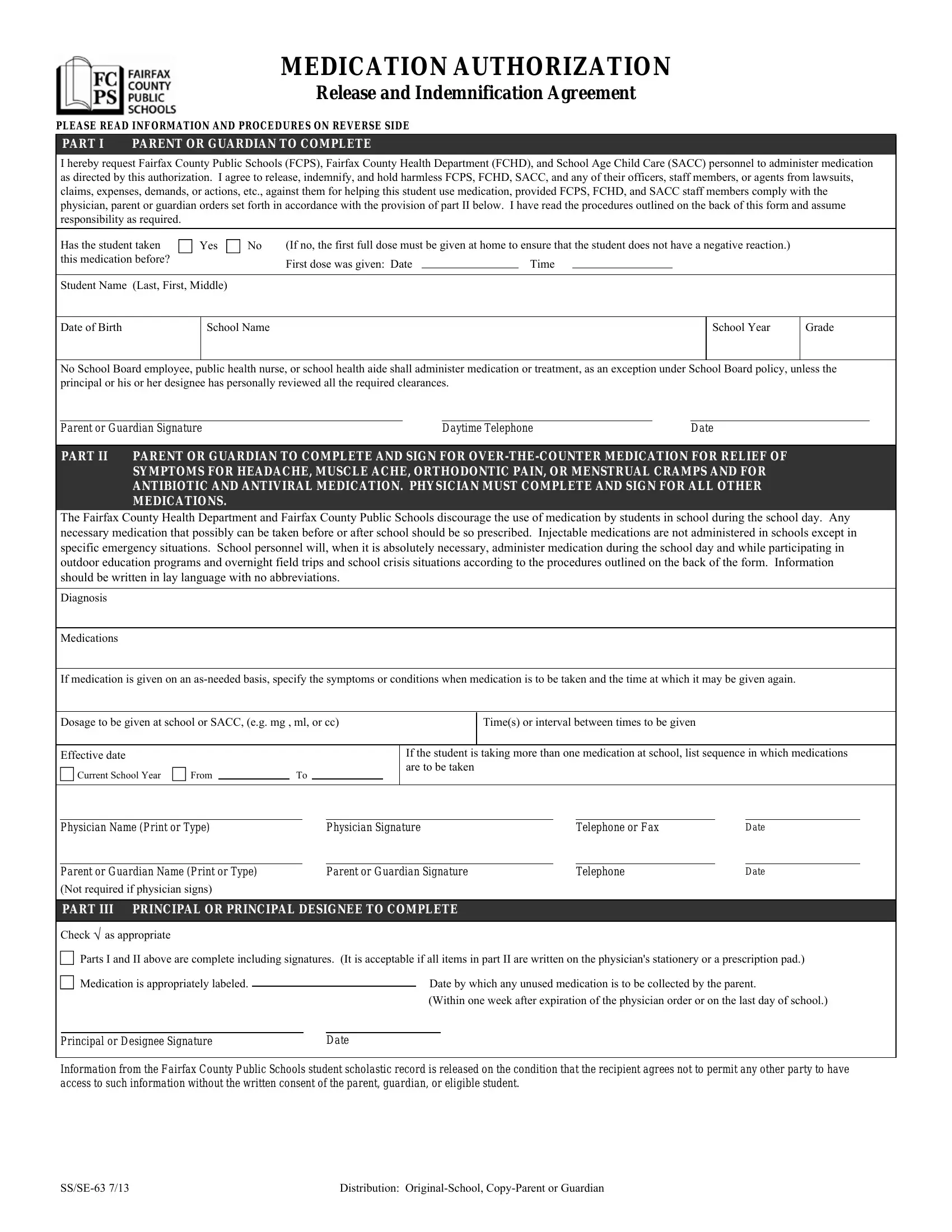
Fairfax Medication Authorization PDF Form FormsPal
Failure to complete this form in its entirety may result in delayed processing or an adverse. I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the.
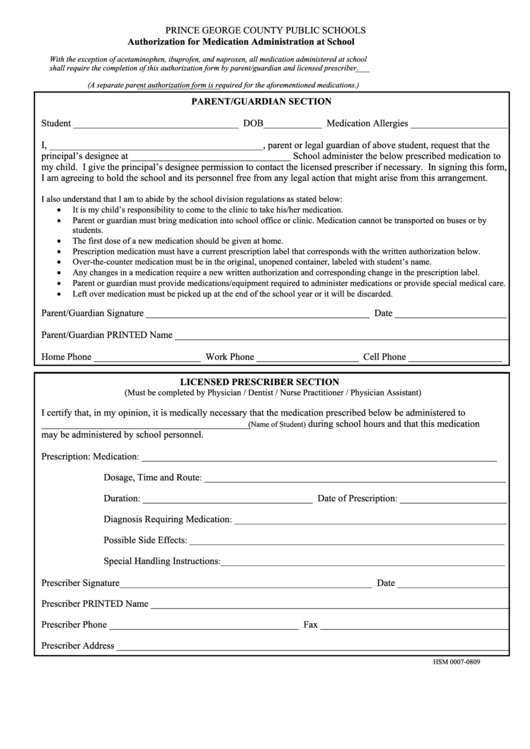
Authorization For Medication Administration At School Form Printable
I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. This form is based on express scripts standard criteria and may not.

Fillable Online medication administration authorization form Fax Email
I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. This form is based on express scripts standard criteria and may not.
Medication Administration/medical Authorization And Release Form
This form is based on express scripts standard criteria and may not be applicable to all patients; Certain plans and situations may require. I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. Failure to complete this form in its entirety may result in delayed processing.
Fillable Online ADMINISTRATION OF MEDICATION AUTHORIZATION Fax Email
I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. This form is based on express scripts standard criteria and may not be applicable to all patients; Certain plans and situations may require. I understand that the health plan, insurer, medical group or its designees may.
Certain Plans And Situations May Require.
Failure to complete this form in its entirety may result in delayed processing or an adverse. This form is based on express scripts standard criteria and may not be applicable to all patients; I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to. I understand that the health plan, insurer, medical group or its designees may perform a routine audit and request the medical information necessary to.