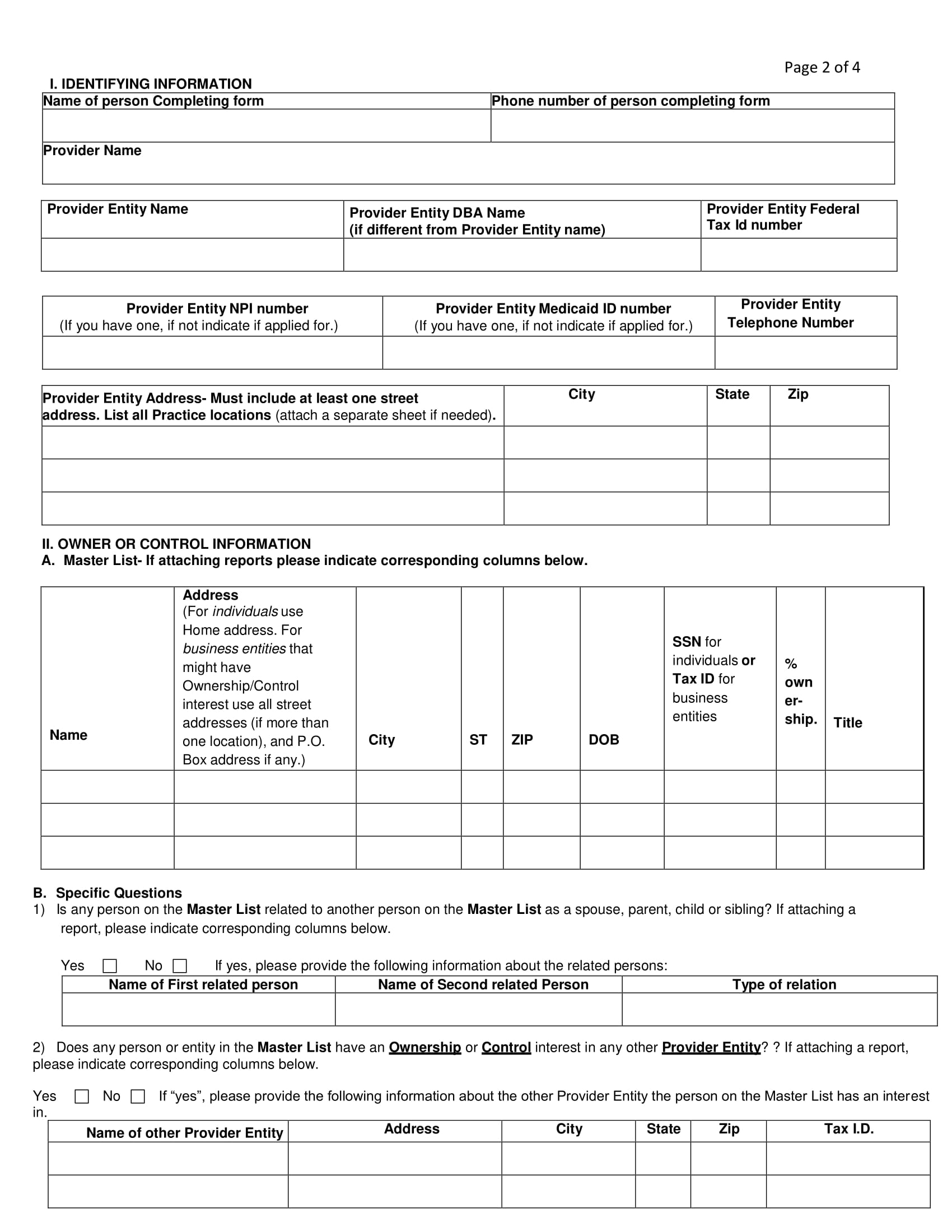
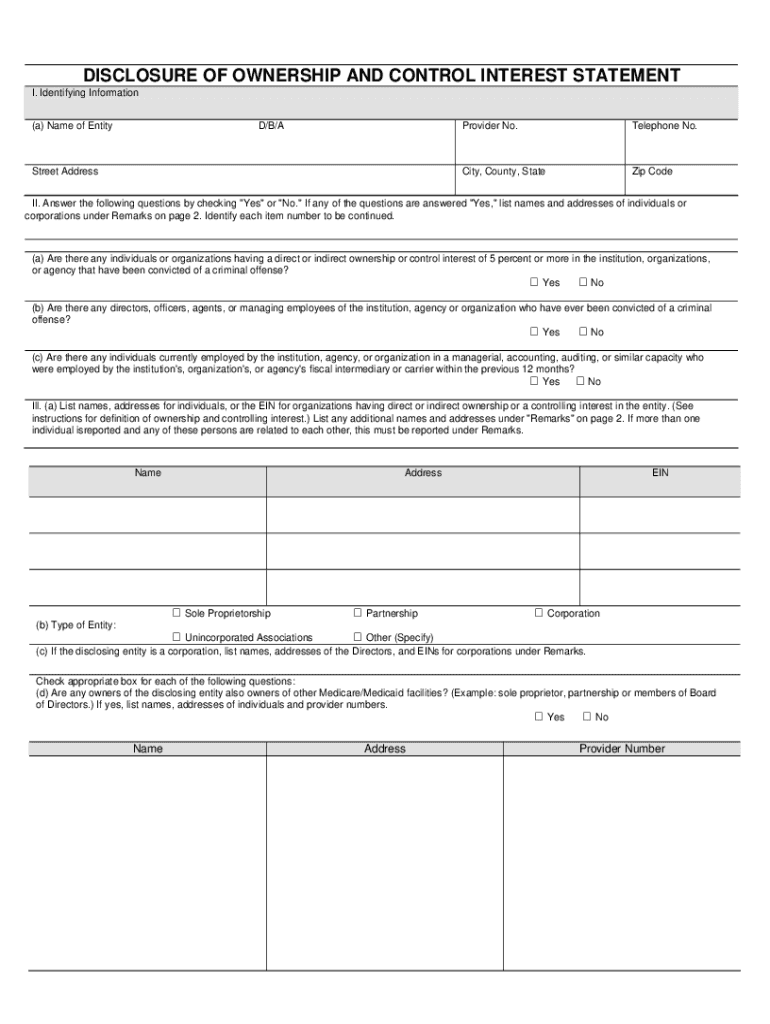
Disclosure Of Ownership Form - For individuals, list the name, title, address, date of birth (dob) and social security number (ssn) for each individual having an ownership or control. The disclosing entity is required to fully disclose all levels of ownership of 5% or more, and to fully disclose all entities and all individuals at each. Any authorized/designated representative of the provider/disclosing entity may complete and sign this form on behalf of the provider/disclosing. Providers participating in medicaid and/or chip managed care networks must complete and submit the disclosure statement below in accordance. Nstructions for completing the disclosure of ownership and control interest statement completion and submission of this.
For individuals, list the name, title, address, date of birth (dob) and social security number (ssn) for each individual having an ownership or control. Nstructions for completing the disclosure of ownership and control interest statement completion and submission of this. Any authorized/designated representative of the provider/disclosing entity may complete and sign this form on behalf of the provider/disclosing. Providers participating in medicaid and/or chip managed care networks must complete and submit the disclosure statement below in accordance. The disclosing entity is required to fully disclose all levels of ownership of 5% or more, and to fully disclose all entities and all individuals at each.
For individuals, list the name, title, address, date of birth (dob) and social security number (ssn) for each individual having an ownership or control. The disclosing entity is required to fully disclose all levels of ownership of 5% or more, and to fully disclose all entities and all individuals at each. Any authorized/designated representative of the provider/disclosing entity may complete and sign this form on behalf of the provider/disclosing. Providers participating in medicaid and/or chip managed care networks must complete and submit the disclosure statement below in accordance. Nstructions for completing the disclosure of ownership and control interest statement completion and submission of this.
Fillable Online Provider Disclosure of Ownership and Control Interest
For individuals, list the name, title, address, date of birth (dob) and social security number (ssn) for each individual having an ownership or control. Nstructions for completing the disclosure of ownership and control interest statement completion and submission of this. Providers participating in medicaid and/or chip managed care networks must complete and submit the disclosure statement below in accordance. The.

Fillable Online Disclosure of Ownership and Control Interest Statement
The disclosing entity is required to fully disclose all levels of ownership of 5% or more, and to fully disclose all entities and all individuals at each. Providers participating in medicaid and/or chip managed care networks must complete and submit the disclosure statement below in accordance. Nstructions for completing the disclosure of ownership and control interest statement completion and submission.
FREE 15+ Legal Ownership Form Samples, PDF, MS Word, Google Docs
Nstructions for completing the disclosure of ownership and control interest statement completion and submission of this. Any authorized/designated representative of the provider/disclosing entity may complete and sign this form on behalf of the provider/disclosing. The disclosing entity is required to fully disclose all levels of ownership of 5% or more, and to fully disclose all entities and all individuals at.

Fillable Online
The disclosing entity is required to fully disclose all levels of ownership of 5% or more, and to fully disclose all entities and all individuals at each. Nstructions for completing the disclosure of ownership and control interest statement completion and submission of this. Any authorized/designated representative of the provider/disclosing entity may complete and sign this form on behalf of the.
Ownership Disclosure Form Fill online with Lumin
Providers participating in medicaid and/or chip managed care networks must complete and submit the disclosure statement below in accordance. Nstructions for completing the disclosure of ownership and control interest statement completion and submission of this. The disclosing entity is required to fully disclose all levels of ownership of 5% or more, and to fully disclose all entities and all individuals.
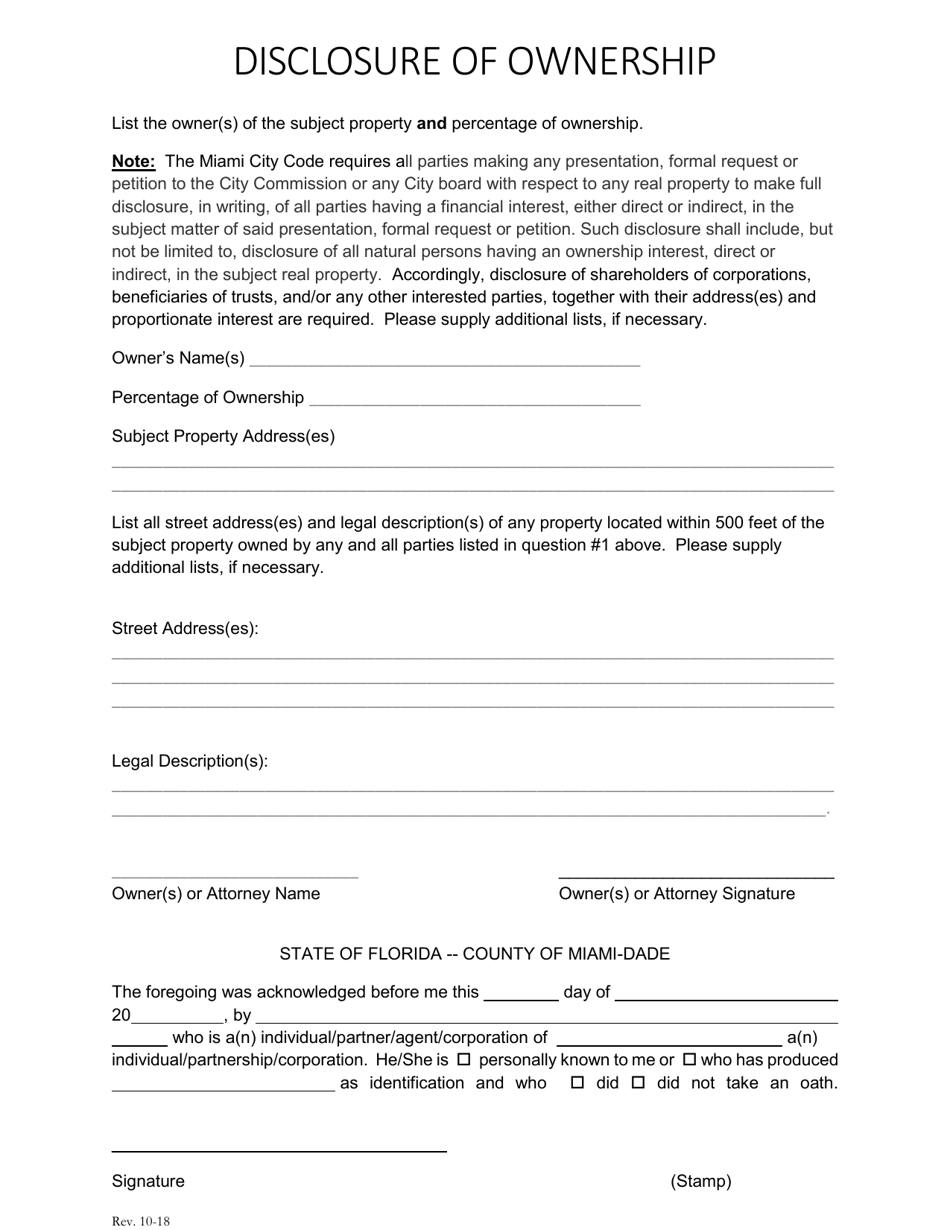
City of Miami, Florida Disclosure of Ownership Fill Out, Sign Online
The disclosing entity is required to fully disclose all levels of ownership of 5% or more, and to fully disclose all entities and all individuals at each. Providers participating in medicaid and/or chip managed care networks must complete and submit the disclosure statement below in accordance. Any authorized/designated representative of the provider/disclosing entity may complete and sign this form on.
Disclosure of ownership form template Fill out & sign online DocHub
For individuals, list the name, title, address, date of birth (dob) and social security number (ssn) for each individual having an ownership or control. Any authorized/designated representative of the provider/disclosing entity may complete and sign this form on behalf of the provider/disclosing. Providers participating in medicaid and/or chip managed care networks must complete and submit the disclosure statement below in.
Ahcccs Control Fill Online, Printable, Fillable, Blank pdfFiller
The disclosing entity is required to fully disclose all levels of ownership of 5% or more, and to fully disclose all entities and all individuals at each. Nstructions for completing the disclosure of ownership and control interest statement completion and submission of this. Providers participating in medicaid and/or chip managed care networks must complete and submit the disclosure statement below.

Cms Disclosure Of Ownership Form Printable Blank PDF Online
The disclosing entity is required to fully disclose all levels of ownership of 5% or more, and to fully disclose all entities and all individuals at each. Providers participating in medicaid and/or chip managed care networks must complete and submit the disclosure statement below in accordance. Nstructions for completing the disclosure of ownership and control interest statement completion and submission.
Fillable Online Disclosure of Ownership and Control Provider
Providers participating in medicaid and/or chip managed care networks must complete and submit the disclosure statement below in accordance. Any authorized/designated representative of the provider/disclosing entity may complete and sign this form on behalf of the provider/disclosing. Nstructions for completing the disclosure of ownership and control interest statement completion and submission of this. The disclosing entity is required to fully.
Any Authorized/Designated Representative Of The Provider/Disclosing Entity May Complete And Sign This Form On Behalf Of The Provider/Disclosing.
Nstructions for completing the disclosure of ownership and control interest statement completion and submission of this. For individuals, list the name, title, address, date of birth (dob) and social security number (ssn) for each individual having an ownership or control. The disclosing entity is required to fully disclose all levels of ownership of 5% or more, and to fully disclose all entities and all individuals at each. Providers participating in medicaid and/or chip managed care networks must complete and submit the disclosure statement below in accordance.