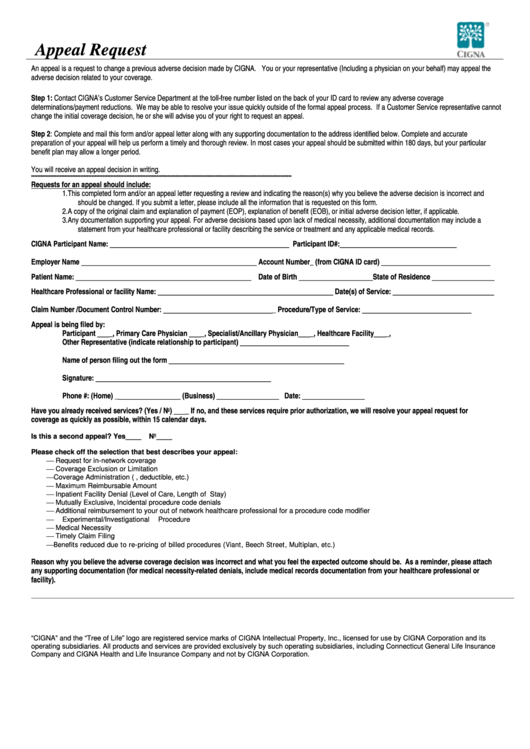
Cigna Appeal Form - This completed form and/or an appeal letter requesting a review and indicating the reason(s) why you believe the adverse decision is incorrect and. The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely review of the appeal. If no additional documentation is required for your appeal or reconsideration request, fax in only this completed coversheet. Complete and mail this form and/or appeal letter along with any supporting documentation to the address identified below. Easily access the cigna appeal form to challenge decisions on claims. You may use the space.
Easily access the cigna appeal form to challenge decisions on claims. The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely review of the appeal. Complete and mail this form and/or appeal letter along with any supporting documentation to the address identified below. You may use the space. If no additional documentation is required for your appeal or reconsideration request, fax in only this completed coversheet. This completed form and/or an appeal letter requesting a review and indicating the reason(s) why you believe the adverse decision is incorrect and.
This completed form and/or an appeal letter requesting a review and indicating the reason(s) why you believe the adverse decision is incorrect and. Complete and mail this form and/or appeal letter along with any supporting documentation to the address identified below. You may use the space. If no additional documentation is required for your appeal or reconsideration request, fax in only this completed coversheet. The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely review of the appeal. Easily access the cigna appeal form to challenge decisions on claims.

Fillable Online Medicare Advantage Provider Appeal Form Fax Email Print
The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely review of the appeal. Easily access the cigna appeal form to challenge decisions on claims. Complete and mail this form and/or appeal letter along with any supporting documentation to the address identified below. You may use the space. This.
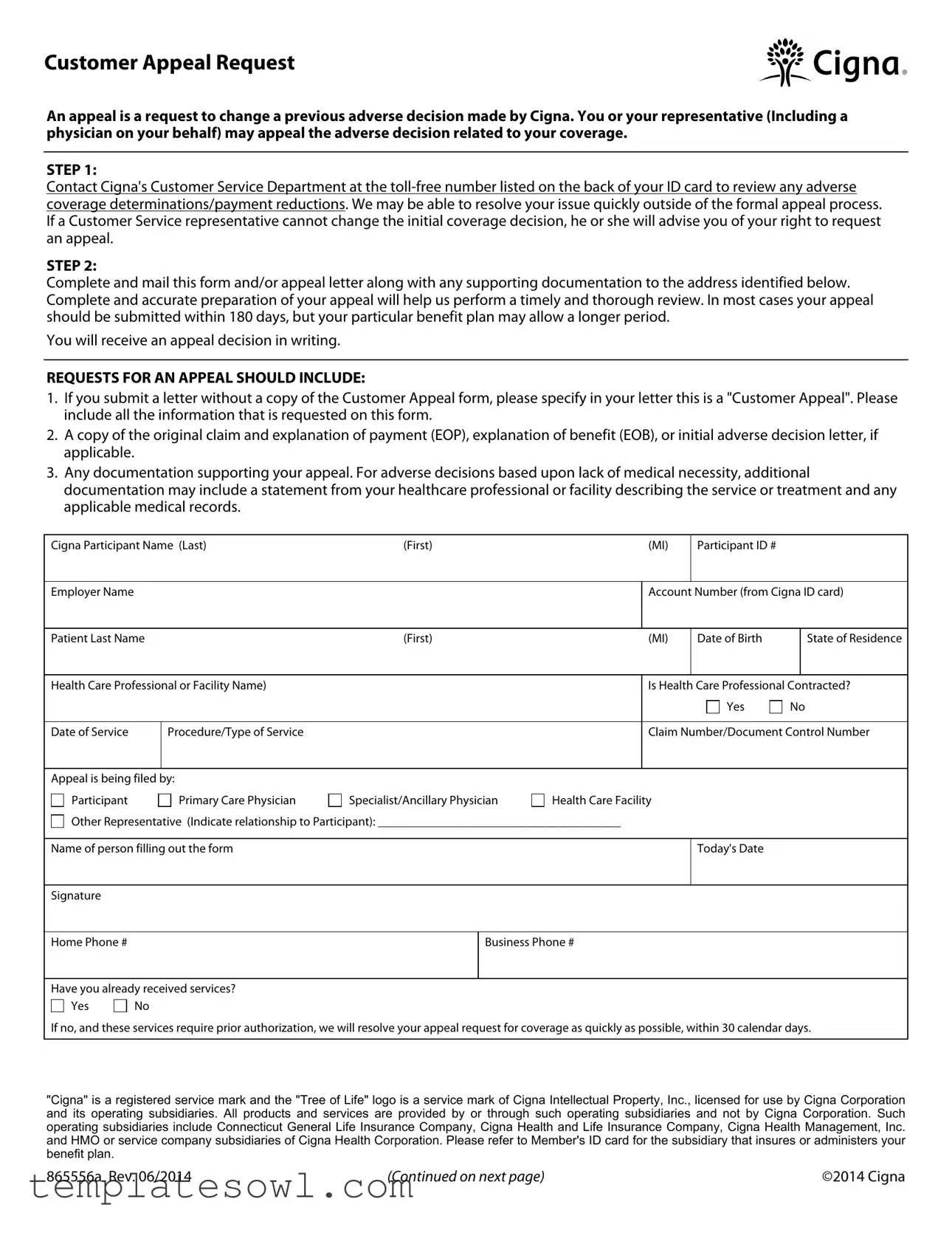
Download Cigna Appeal Form • TemplatesOwl
If no additional documentation is required for your appeal or reconsideration request, fax in only this completed coversheet. Complete and mail this form and/or appeal letter along with any supporting documentation to the address identified below. You may use the space. This completed form and/or an appeal letter requesting a review and indicating the reason(s) why you believe the adverse.
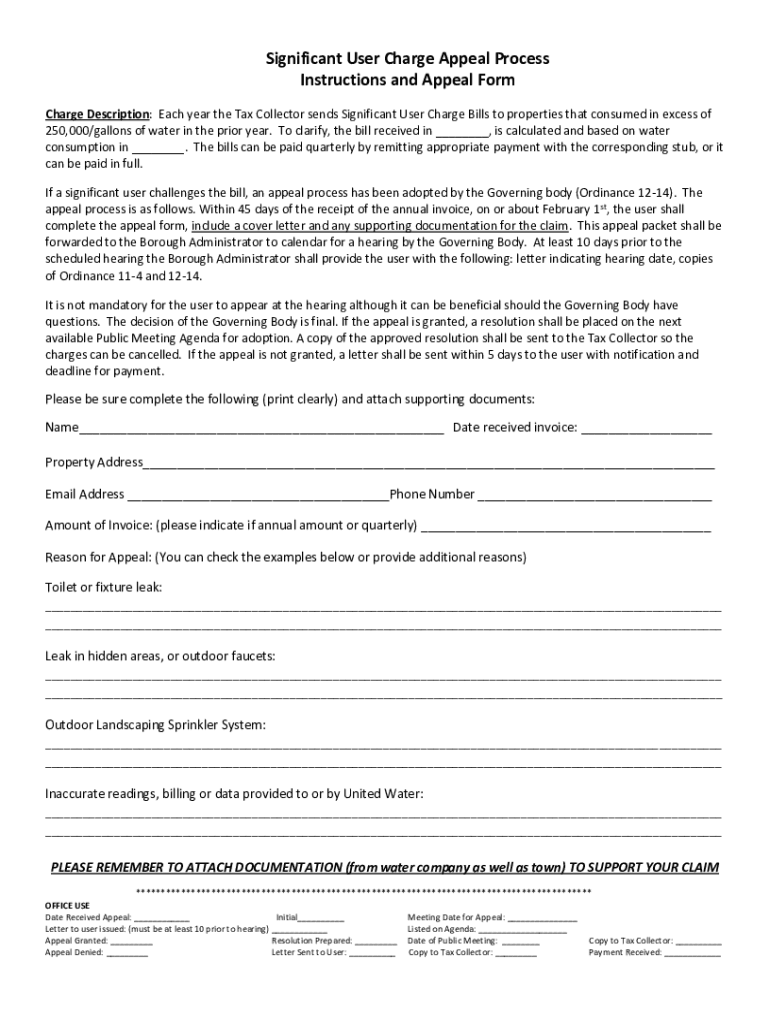
Ides Appeal Form Pdf
If no additional documentation is required for your appeal or reconsideration request, fax in only this completed coversheet. The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely review of the appeal. Easily access the cigna appeal form to challenge decisions on claims. This completed form and/or an appeal.
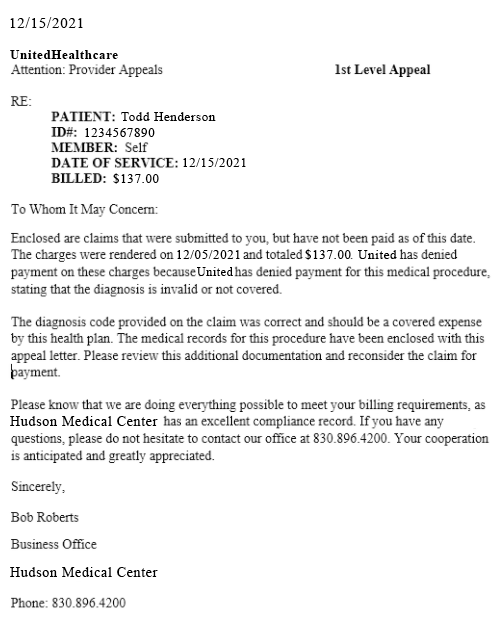
5 Sample Appeal Letters for Medical Claim Denials That Actually Work
Easily access the cigna appeal form to challenge decisions on claims. Complete and mail this form and/or appeal letter along with any supporting documentation to the address identified below. You may use the space. This completed form and/or an appeal letter requesting a review and indicating the reason(s) why you believe the adverse decision is incorrect and. The form will.
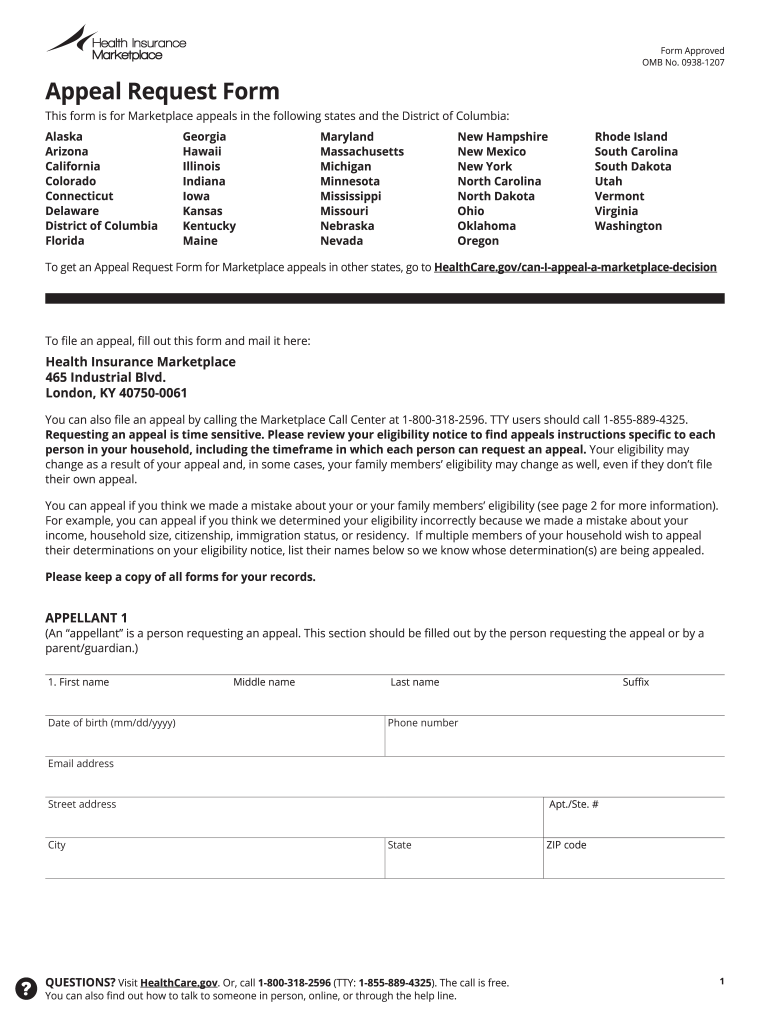
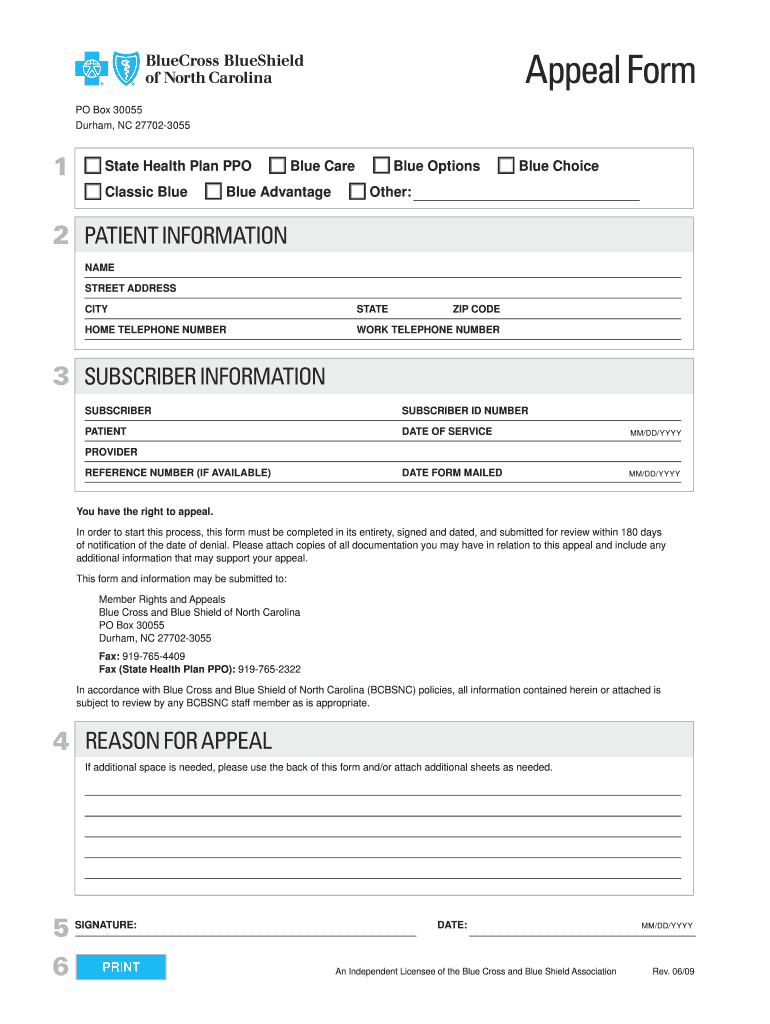
Healthcare Forms Appeal Fill Online Printable Fillable Blank
If no additional documentation is required for your appeal or reconsideration request, fax in only this completed coversheet. This completed form and/or an appeal letter requesting a review and indicating the reason(s) why you believe the adverse decision is incorrect and. Easily access the cigna appeal form to challenge decisions on claims. Complete and mail this form and/or appeal letter.
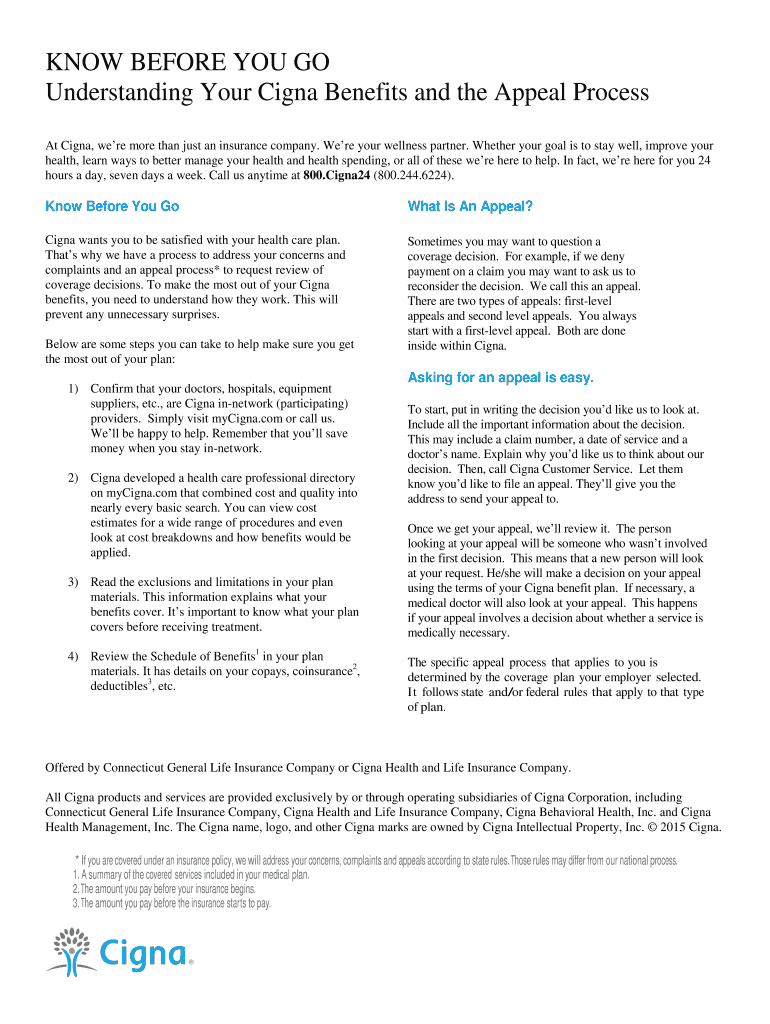
Fillable Online Understanding Your Cigna Benefits and the Appeal
Complete and mail this form and/or appeal letter along with any supporting documentation to the address identified below. This completed form and/or an appeal letter requesting a review and indicating the reason(s) why you believe the adverse decision is incorrect and. You may use the space. If no additional documentation is required for your appeal or reconsideration request, fax in.
Fillable Online Medical Claim Appeal Form 08 P421 Interactive Revised
You may use the space. If no additional documentation is required for your appeal or reconsideration request, fax in only this completed coversheet. Complete and mail this form and/or appeal letter along with any supporting documentation to the address identified below. The form will help to fully document the circumstances around the appeal request and will also help to ensure.
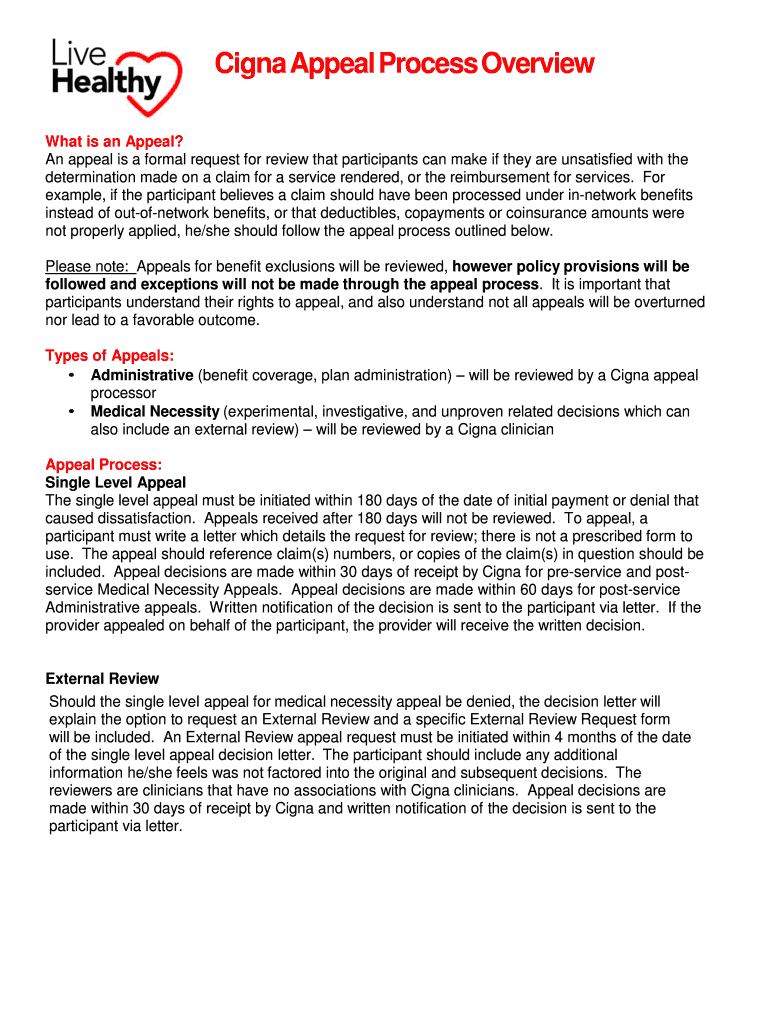
Fillable Online Cigna Appeal Process Overview Fax Email Print pdfFiller
This completed form and/or an appeal letter requesting a review and indicating the reason(s) why you believe the adverse decision is incorrect and. You may use the space. Easily access the cigna appeal form to challenge decisions on claims. If no additional documentation is required for your appeal or reconsideration request, fax in only this completed coversheet. Complete and mail.
Top 5 Cigna Prior Authorization Form Templates free to download in PDF
Complete and mail this form and/or appeal letter along with any supporting documentation to the address identified below. Easily access the cigna appeal form to challenge decisions on claims. If no additional documentation is required for your appeal or reconsideration request, fax in only this completed coversheet. This completed form and/or an appeal letter requesting a review and indicating the.

Top United Healthcare Appeal Form Templates Free To Download In PDF
You may use the space. Easily access the cigna appeal form to challenge decisions on claims. This completed form and/or an appeal letter requesting a review and indicating the reason(s) why you believe the adverse decision is incorrect and. The form will help to fully document the circumstances around the appeal request and will also help to ensure a timely.
This Completed Form And/Or An Appeal Letter Requesting A Review And Indicating The Reason(S) Why You Believe The Adverse Decision Is Incorrect And.
If no additional documentation is required for your appeal or reconsideration request, fax in only this completed coversheet. Easily access the cigna appeal form to challenge decisions on claims. You may use the space. Complete and mail this form and/or appeal letter along with any supporting documentation to the address identified below.