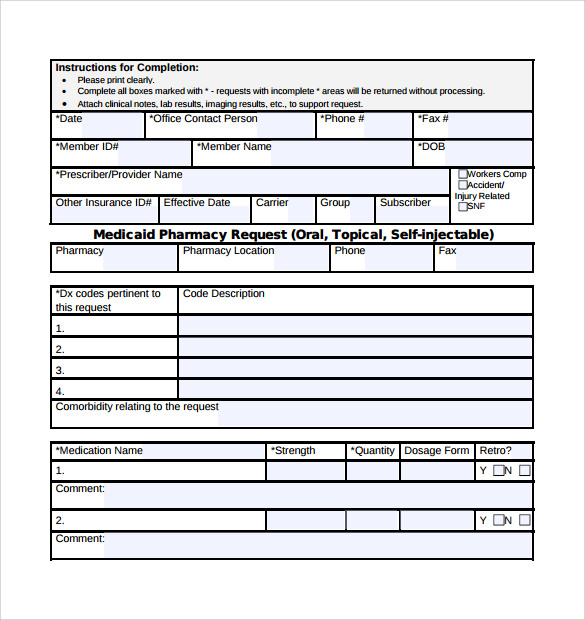
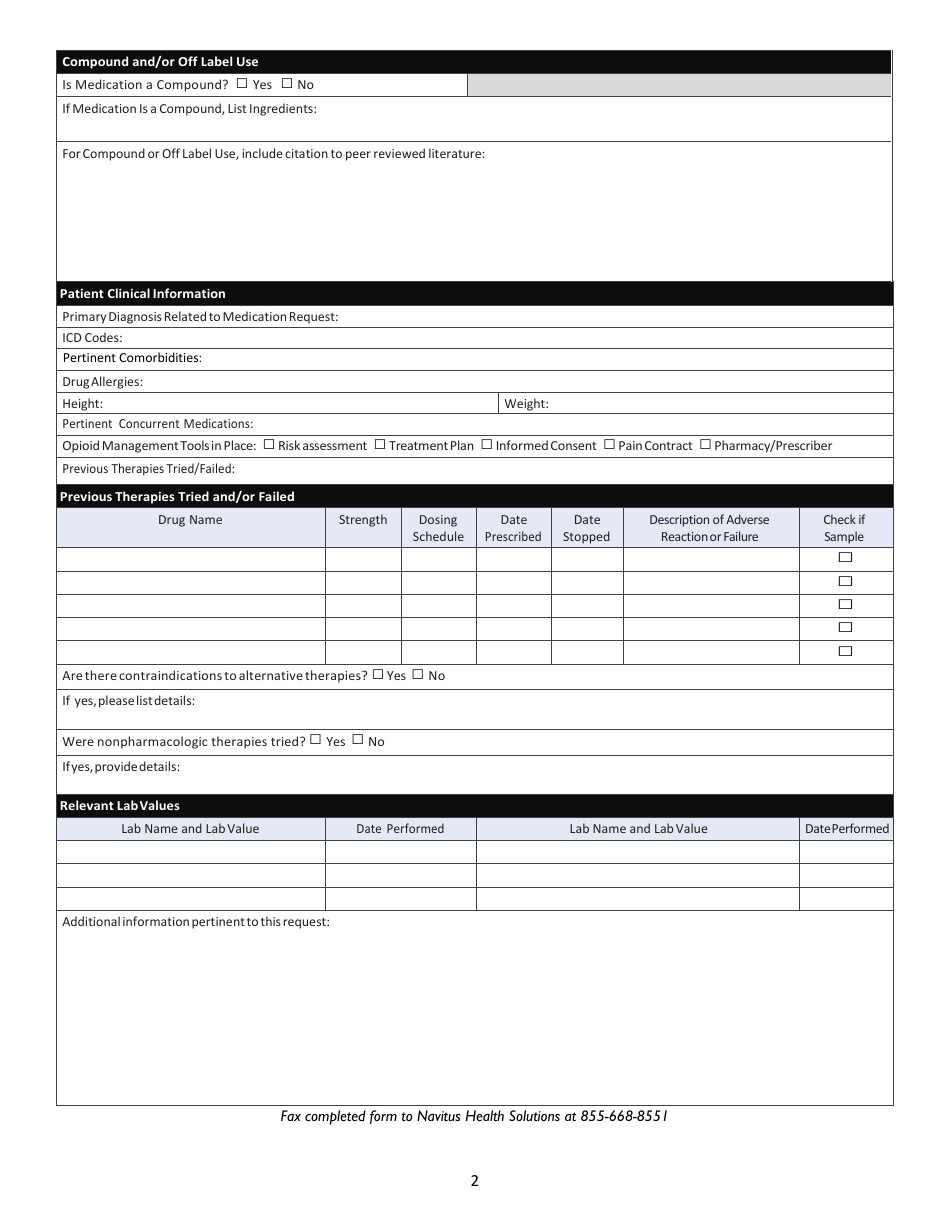
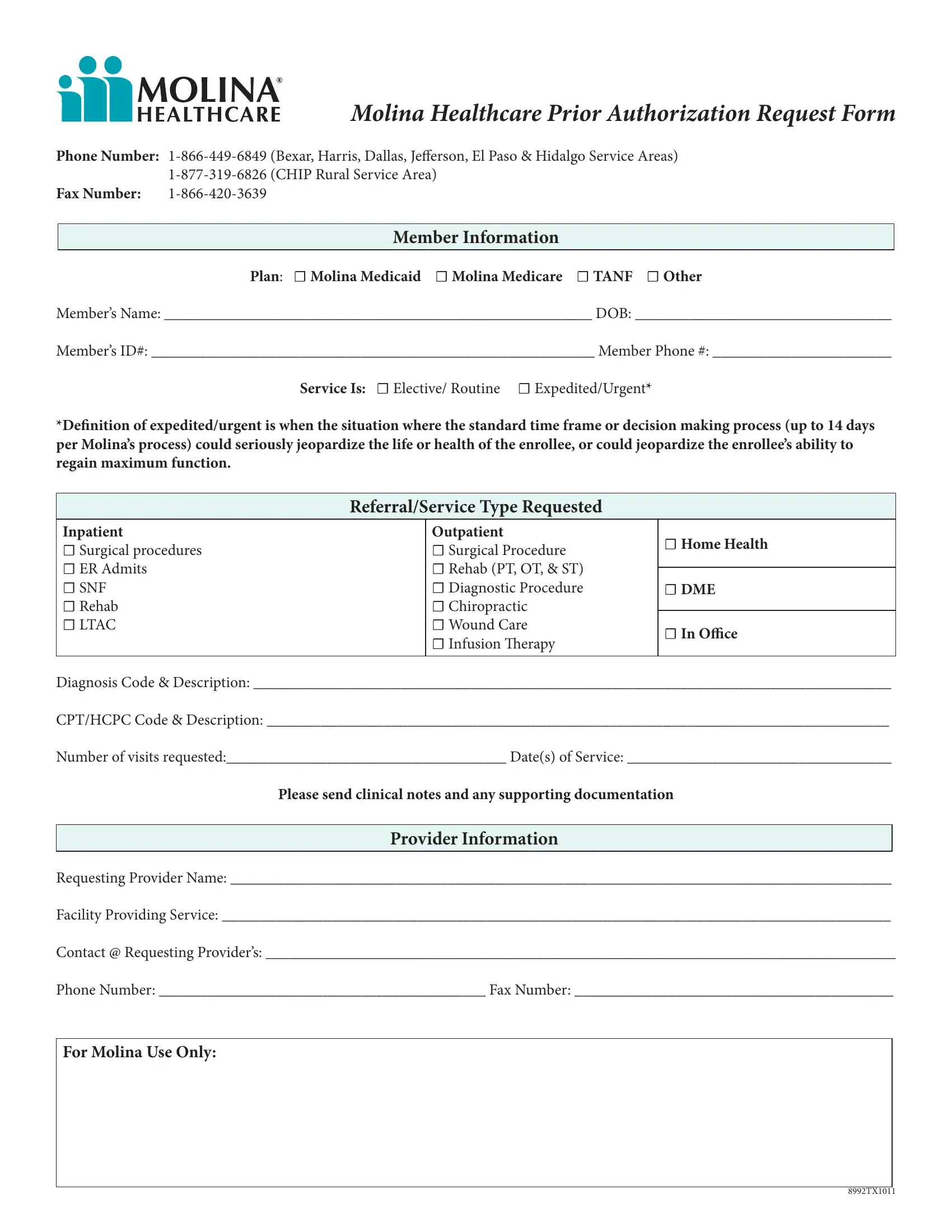
Arkansas Medicaid Prior Authorization Form - Write the name of the medicaid provider requesting prior authorization. Member must be eligible at the time services are rendered. Others are added as they become available. Some of the forms used by arkansas medicaid and its providers are available in electronic format. Use one form per beneficiary please. Services must be a covered health plan benefit and medically necessary with prior. Please attach or include a letter of medical necessity along with supporting documentation (e.g.
Please attach or include a letter of medical necessity along with supporting documentation (e.g. Some of the forms used by arkansas medicaid and its providers are available in electronic format. Others are added as they become available. Member must be eligible at the time services are rendered. Use one form per beneficiary please. Write the name of the medicaid provider requesting prior authorization. Services must be a covered health plan benefit and medically necessary with prior.
Others are added as they become available. Use one form per beneficiary please. Some of the forms used by arkansas medicaid and its providers are available in electronic format. Please attach or include a letter of medical necessity along with supporting documentation (e.g. Member must be eligible at the time services are rendered. Services must be a covered health plan benefit and medically necessary with prior. Write the name of the medicaid provider requesting prior authorization.
FREE 7+ Medicaid Prior Authorization Forms in PDF
Use one form per beneficiary please. Some of the forms used by arkansas medicaid and its providers are available in electronic format. Services must be a covered health plan benefit and medically necessary with prior. Please attach or include a letter of medical necessity along with supporting documentation (e.g. Write the name of the medicaid provider requesting prior authorization.
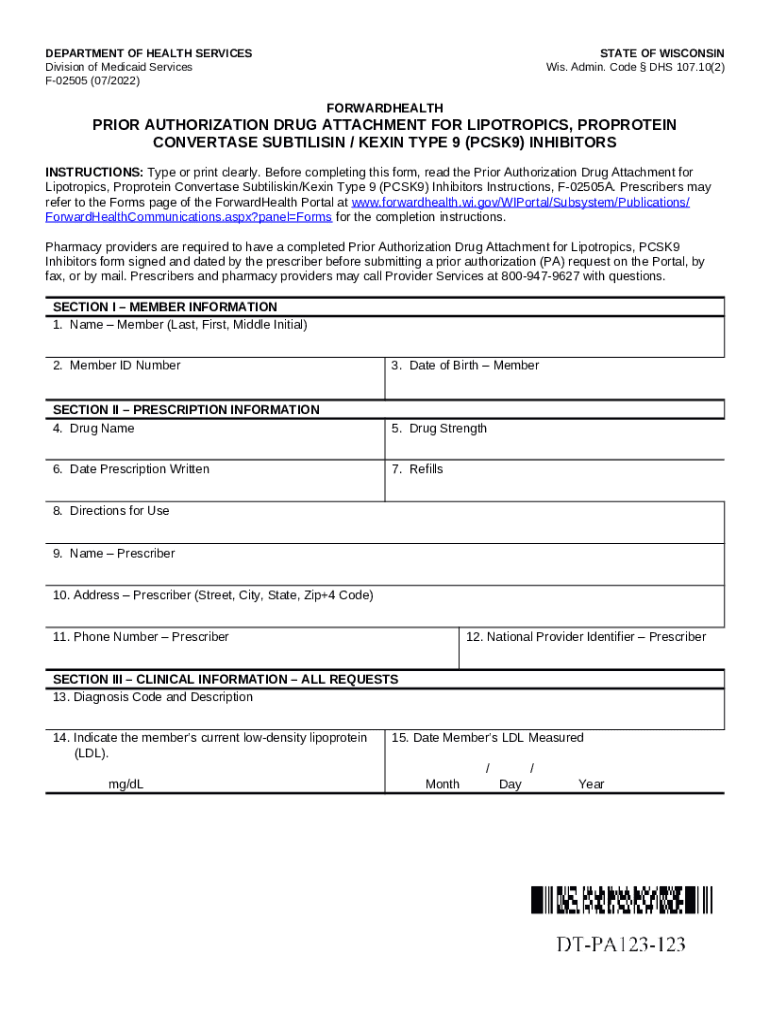
Prior Authorization Preferred Drug List ForwardHealth Portal dhs
Write the name of the medicaid provider requesting prior authorization. Services must be a covered health plan benefit and medically necessary with prior. Please attach or include a letter of medical necessity along with supporting documentation (e.g. Member must be eligible at the time services are rendered. Some of the forms used by arkansas medicaid and its providers are available.

20202025 Form AR Medicaid Prior Authorization Request Fill Online
Member must be eligible at the time services are rendered. Others are added as they become available. Use one form per beneficiary please. Some of the forms used by arkansas medicaid and its providers are available in electronic format. Write the name of the medicaid provider requesting prior authorization.
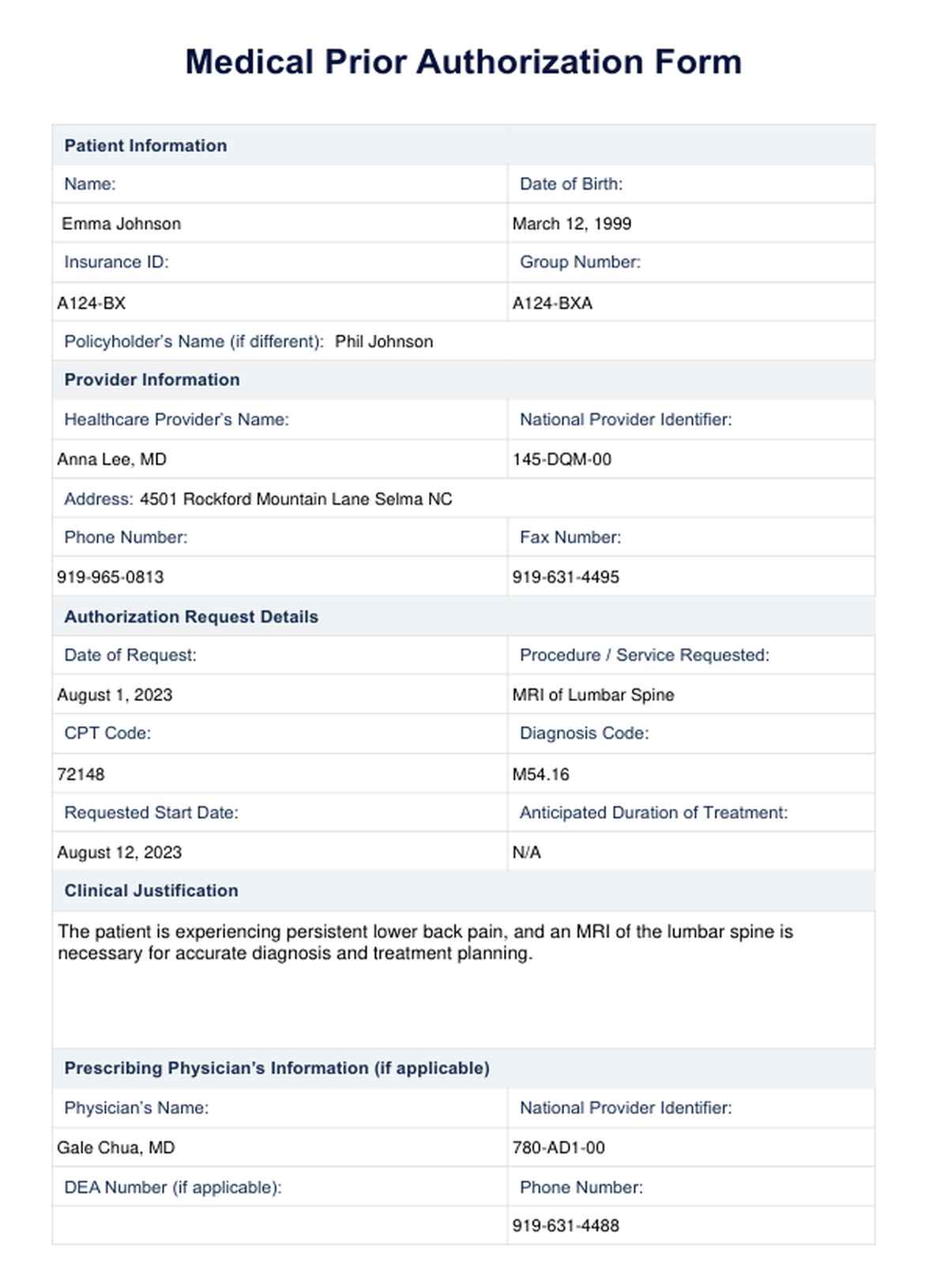
Prior Authorization Form Pdf
Please attach or include a letter of medical necessity along with supporting documentation (e.g. Use one form per beneficiary please. Others are added as they become available. Member must be eligible at the time services are rendered. Write the name of the medicaid provider requesting prior authorization.
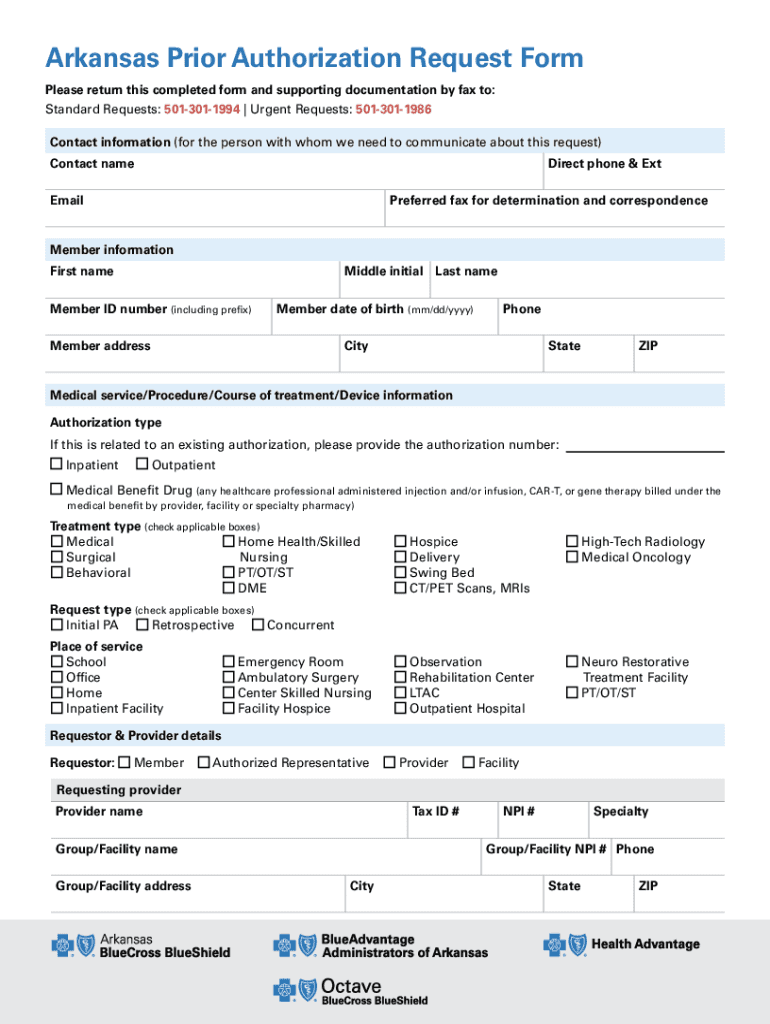
Fillable Online Arkansas Prior Authorization Request Form Fax Email
Use one form per beneficiary please. Please attach or include a letter of medical necessity along with supporting documentation (e.g. Others are added as they become available. Member must be eligible at the time services are rendered. Some of the forms used by arkansas medicaid and its providers are available in electronic format.
Arkansas Prescription Drug Prior Authorization Form Fill Out, Sign
Please attach or include a letter of medical necessity along with supporting documentation (e.g. Use one form per beneficiary please. Member must be eligible at the time services are rendered. Services must be a covered health plan benefit and medically necessary with prior. Some of the forms used by arkansas medicaid and its providers are available in electronic format.
Health PDF Forms Fillable and Printable
Others are added as they become available. Use one form per beneficiary please. Some of the forms used by arkansas medicaid and its providers are available in electronic format. Write the name of the medicaid provider requesting prior authorization. Member must be eligible at the time services are rendered.
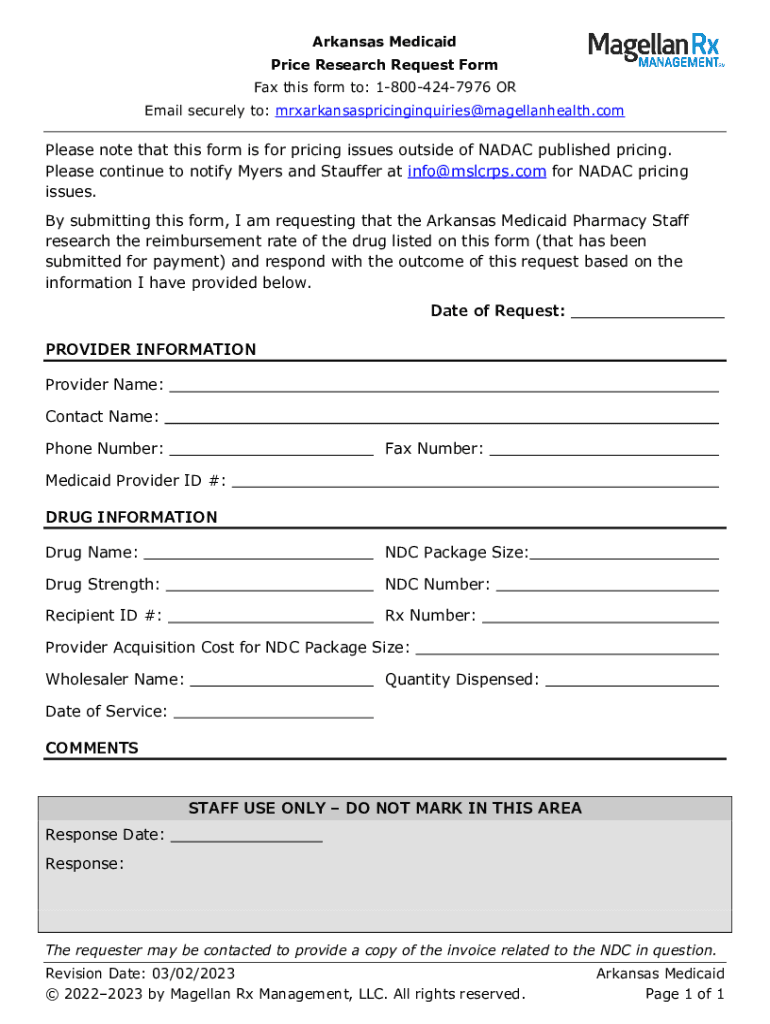
Fillable Online Arkansas Medicaid Price Research Request Form. Arkansas
Please attach or include a letter of medical necessity along with supporting documentation (e.g. Some of the forms used by arkansas medicaid and its providers are available in electronic format. Member must be eligible at the time services are rendered. Others are added as they become available. Services must be a covered health plan benefit and medically necessary with prior.
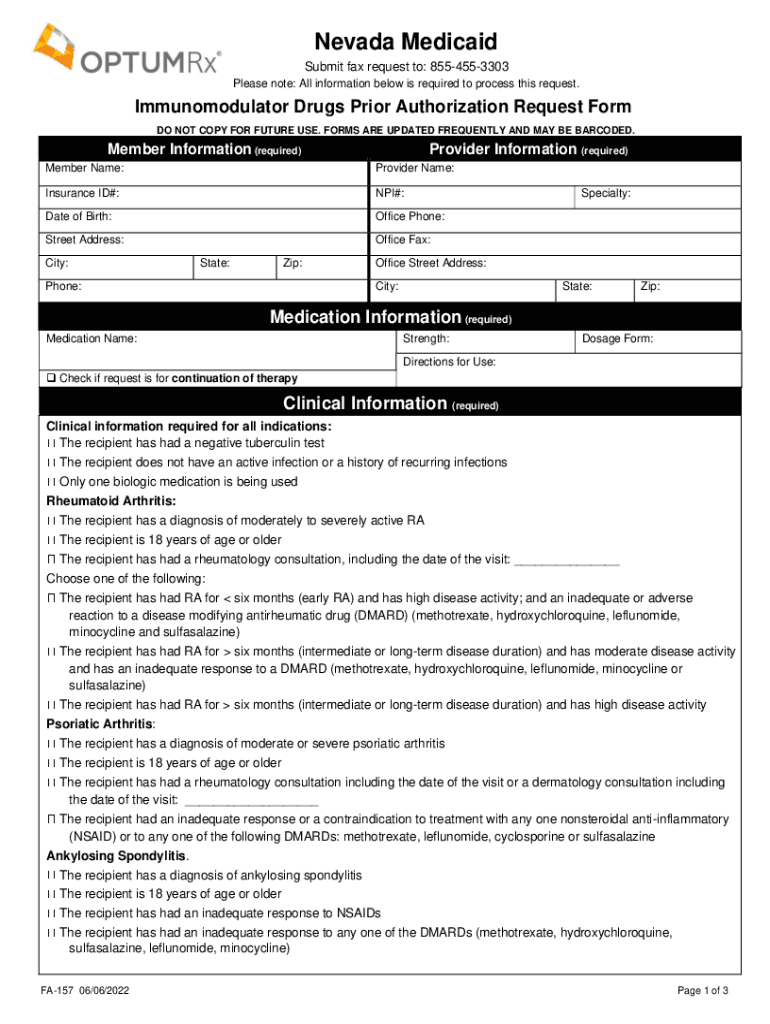
Fillable Online Free Nevada Medicaid Prior Authorization Form PDF
Services must be a covered health plan benefit and medically necessary with prior. Others are added as they become available. Write the name of the medicaid provider requesting prior authorization. Use one form per beneficiary please. Some of the forms used by arkansas medicaid and its providers are available in electronic format.

Free Mississippi Medicaid Prior Rx Authorization Form PDF EForms
Member must be eligible at the time services are rendered. Please attach or include a letter of medical necessity along with supporting documentation (e.g. Use one form per beneficiary please. Write the name of the medicaid provider requesting prior authorization. Others are added as they become available.
Write The Name Of The Medicaid Provider Requesting Prior Authorization.
Others are added as they become available. Please attach or include a letter of medical necessity along with supporting documentation (e.g. Some of the forms used by arkansas medicaid and its providers are available in electronic format. Services must be a covered health plan benefit and medically necessary with prior.
Member Must Be Eligible At The Time Services Are Rendered.
Use one form per beneficiary please.